
I know why I got celiac disease. Do you?
We all have our special origin stories when it comes to why we are the way we are. Humans love to reach back through the strands of our past and attempt to reweave them retrospectively into a narrative we can understand. “X happened, and Y happened, and Z happened” isn’t an appealing way to view our life story: it’s disorganized and random. “X happened, and therefore Y happened, and it all came to a head with Z” is neater and much more satisfying.
So, I know why I have celiac—or, at least, I like to believe I do. I’ve taken all my precious, faulty memories and molded them into a story that makes sense.
My Theory
It’s simple enough: I was born with the celiac gene and lived happily in my glutenous environment, eating whatever I darn well pleased, without so much as a twinge from my cast-iron stomach. Then, I lost sixty pounds in a year, messing with my gut bacteria in ways not even scientists understand. Immediately after I stopped losing and started maintaining, I got sick. Eventually, I learned it was celiac.
To me, the timing is too coincidental to be coincidence. Thus, with no hard evidence whatsoever, I’m convinced: I wreaked havoc on my body’s bacteria, then I gave them some gluten and ruined everything—all in pursuit of thinness. (How many pounds my body has reacquired in revenge is not an important part of the story.)
“But Molly,” you may protest, “I’m a naturally svelte god/goddess who has never actively tried to lose a pound in my life, yet I too have celiac disease. How can this be?”
If that’s so, then after mumbling something less polite, I would thank you for the insightful question, because it leads nicely into the second half of my post.
The Pie Theory
One of the best parts of the recent Columbia conference was Dr. Benjamin Lebwohl’s discussion of causal pies. This is a yummier name for a fundamental principle of epidemiology known as “the sufficient-cause model.” According to it, multiple risk factors for a disease come together in one person, like pieces of a pie. Once the sufficient factors (or ingredients) are there, the person gets the disease.
However, more than one set of ingredients can be combined to make a pie (as any gluten-free baker who has ever had to choose between all-purpose blends knows all too well). Similarly, most diseases have more than one sufficient cause; there’s more than one way to develop them.
For celiac disease to develop, two pieces of the pie must be there: genes (HLA DQ2 or DQ8), and gluten. But by themselves, they’re insufficient cause; almost a third of the US population has the gene and eats gluten, but most of them don’t have celiac. (There could be other universally necessary causes, but no one’s found them yet.) The rest of the pie needs to be filled in, perhaps completely differently for you and for me, with other causes.
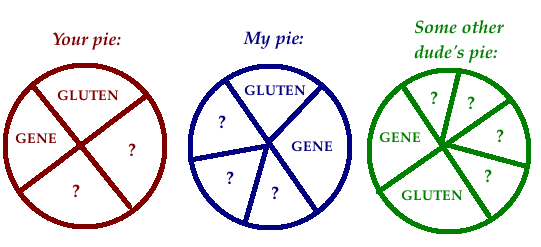 The other pieces might include:
The other pieces might include:
- early OR late gluten introduction by parents (which I have complained about before)
- spring or summer birthday (because you probably started eating gluten in the winter, when infections were going around)
- microbiotic dysbiosis (messed-up gut bacteria)
- antibiotic usage (possibly insofar as it contributes to the above)
- GMOs (but I doubt it. As Dr. Alessio Fasano pointed out, “There are no GMOs in Europe, but we still have celiac disease!”)
- leaky gut (which Dr. Fasano talks up in his new book, Gluten Freedom)
- headache medication (possibly because it makes your gut leak; the aspirin-based ones I regularly overused in high school before discovering caffeine are not included here)
- other autoimmune diseases (though they may in fact be consequences of the same factors as celiac—pies rather than pieces)
- excessive hygiene (which I’ve joked about before)
- and so on.
Why all the theories?
It’s important to determine causes of celiac disease not only because humans hunger for coherent life stories, but also because discovering causes could help us prevent, treat, or even cure future cases. This is particularly crucial because celiac disease is increasing in prevalence.
Plus, differently constructed pies may require different treatments. The baking metaphor breaks down a bit here, but we know that some people take longer to heal than others, and that some people must adopt additional measures beyond the gluten-free diet to get well, while others get cross-contaminated regularly with no consequences. Maybe that’s because their identical disease has different causes.

Original photo of a probably glutenous lemon pie © speedbug | Flickr
Dr. Lebwohl did not make any jokes about a) the gluten content of causal pies, or b) celiac disease being “easy as pie” to develop, so please consider those bad jokes my contribution to the scientific conversation.
Now, it’s your turn to contribute: Why do you think you got celiac disease, or another GRD? Do you have a pet theory about why they are increasing in prevalence?
This is the latest installment in my Sprue/False series of simple but difficult-to-answer questions about celiac disease. (See also Is a Gluten-Free Diet Good Enough? and More on Drugs.) By the way, although “Why do we get other gluten-related disorders?” is a great question too, I focused on celiac because, unfortunately, we’re even farther from answers when it comes to other GRDs.






